What is the anatomical structure of the hip?
The hip joint serves as the connecting articulation between the pelvis and the lower limb. It is formed by the articulation of the femoral head and the acetabulum of the pelvis. The femoral head has a hemispherical shape, whereas the acetabulum is concave. The articular surfaces of both bones are covered with articular cartilage.

The hip joint is formed by the articulation between the femoral head and the acetabulum.
What is hip osteoarthritis?
Hip osteoarthritis is characterized by progressive degeneration of the articular cartilage, ultimately leading to bone-on-bone contact. Typical symptoms include pain, stiffness, gait disturbances (limping), and leg length discrepancy due to joint deformity.
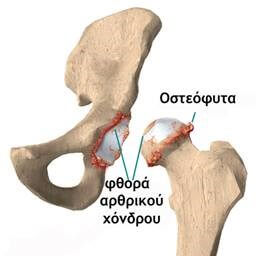
In osteoarthritis, the articular cartilage is destroyed and bony projections called osteophytes develop.
How is hip osteoarthritis managed?
Initial management includes weight reduction, administration of analgesics and anti-inflammatory medications, activity modification, physical therapy, and use of walking aids.
If conservative measures fail to provide sufficient symptom relief and the patient’s quality of life is significantly impaired, surgical intervention becomes indicated.

X-ray of a normal hip (left) and an osteoarthritic hip with loss of articular cartilage and bone-on-bone contact.
What is hip osteoarthritis?
Total arthroplasty aims to replace the worn joint with an artificial one. During the procedure, the worn femoral head is removed to place a specialized stem, while the acetabulum is prepared to receive a hemispherical cup. A metal or ceramic head is placed on the femoral stem, and a polyethylene, ceramic, or metal insert is placed in the acetabular cup.
Usually, the femoral stem is implanted inside the femur without the use of synthetic material (“cement”). The surfaces of the materials are specially treated and coated to facilitate the integration of the implant with the bone.
In some cases, a metal stem is not used in the femur; instead, a special metal cap is placed (surface arthroplasty).
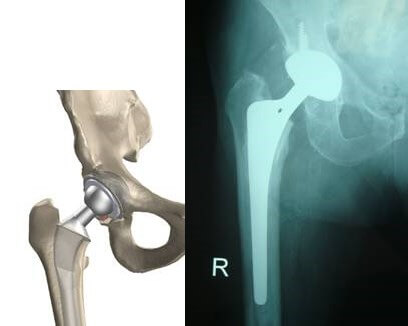
During hip arthroplasty, a metal stem is implanted into the femur and a corresponding metal prosthesis is placed in the acetabulum.
What are the indications for total hip arthroplasty (THA)?
Total hip arthroplasty is recommended for patients with advanced hip osteoarthritis and significant clinical symptoms such as:
- Severe pain limiting work or recreational activities, significantly affecting quality of life
- Moderate to severe pain at rest, either during the day or night
- Pain unresponsive to medications, physical therapy, or use of a cane
- Stiffness causing substantial limitation in range of motion
- Limb deformity
- Adverse effects from long-term medication use
- Failure of conservative treatment
Most patients are over 60 years of age and experience significant pain, particularly during movement, along with functional limitations.
What are the goals of total hip arthroplasty?
The aim of hip arthroplasty is to alleviate pain, improve mobility, and restore function, thereby enhancing the patient’s overall quality of life. After surgery, most patients are able to resume normal daily activities; however, excessive joint loading or high-impact activities are discouraged.
Is it advisable to delay total hip arthroplasty for as long as possible?
This is a common misconception. Performing the procedure earlier in the course of disease yields better functional outcomes. Delaying surgery may reduce quality of life both before and after the procedure, especially since no conservative treatment can halt the progression of osteoarthritis. Furthermore, undergoing surgery at an older age may involve increased risk and complexity.
What are the alternative surgical treatments for hip osteoarthritis?
In less severe cases, hip arthroscopy or corrective osteotomy may be considered. In the past, hip arthrodesis (joint fusion) was used for severe cases.
What are the non-surgical (conservative) treatment options for hip osteoarthritis?
While total hip arthroplasty is the definitive treatment for advanced cases, the following conservative options may be effective for patients with mild symptoms:
- Weight loss
- Modification of physical activity
- Use of analgesics and anti-inflammatory medications
- Physical therapy
and of the hip each year.
What outcomes can patients expect from hip arthroplasty?
Total hip arthroplasty provides pain relief in approximately 95% of patients. It enables individuals to comfortably perform daily activities and, in selected cases, engage in low-impact sports. Most patients regain lost mobility and function.
What components and materials are used in total hip arthroplasty?
A total hip replacement consists of four main components: the acetabular shell, the polyethylene liner, the femoral head, and the femoral stem.
Metal components are typically made of titanium or cobalt-chromium alloys; the liner is made of polyethylene, and the femoral head is constructed from either metal or ceramic.
There are various implant designs, sizes, and material combinations available. In selected patients, customized implants may be created to ensure optimal anatomical fit.

What is the life expectancy of a total hip replacement?
The longevity of the prosthesis depends on several factors, including wear resistance of materials (especially polyethylene), patient activity level, and bone quality. Statistically, implant survival ranges from a few months to over 35 years. On average, 80% of hip replacements last 20 years or longer.
What happens if the prosthesis becomes damaged?
If implant failure occurs, revision surgery may be performed to replace one or more components. This can be done once or even multiple times if necessary.
What preoperative preparation is required for total hip arthroplasty?
Preoperative preparation focuses on optimizing the patient’s general health and physical condition. Improving joint mobility and muscle strength before surgery enhances postoperative recovery.
Preoperative evaluations are conducted by an internist, cardiologist, and anesthesiologist, along with comprehensive laboratory tests to ensure medical and psychological readiness.
Certain medications may need to be discontinued, including anticoagulants (aspirin, Sintrom, Plavix), nonsteroidal anti-inflammatory drugs, and immunosuppressants.
Is blood transfusion necessary during surgery?
In most patients, blood transfusion is not required thanks to modern, minimally invasive surgical techniques and intraoperative blood loss management. Nonetheless, patients are usually asked to arrange for the donation of 1–2 units of blood for safety.
Preoperative hemoglobin levels may be increased by administering erythropoietin—a hormone that stimulates red blood cell production—subcutaneously for 3 weeks before surgery, in combination with iron supplementation.
Some patients may also choose to donate autologous blood between 42 and 7 days prior to surgery for potential use during the procedure.This blood is stored and administered if necessary.
Yes. Intraoperative autologous blood recovery systems are often employed, where blood lost during surgery is collected, filtered, and reinfused into the patient. Additionally, tranexamic acid is commonly administered intraoperatively to reduce bleeding. Postoperatively, wound drainage blood may be reinfused within the first 4–6 hours.
What type of anesthesia is used during total hip replacement?
Epidural anesthesia and analgesia are most commonly used. Under local anesthesia, the anesthesiologist inserts a thin catheter into the epidural space—well away from the spinal nerves—allowing continuous administration of local anesthetic to numb the lower extremities.
This catheter remains in place postoperatively, delivering small doses of anesthetic through an infusion pump to ensure effective pain control. During surgery, additional intravenous sedation may be administered for patient comfort.
What is the procedure for performing hip replacement surgery?
During the procedure, a small surgical incision is made in the hip area, and the femoral neck and head are removed. The acetabulum is slightly enlarged to remove the damaged articular cartilage, and the new metal hemispherical cup and the polyethylene liner are inserted.
The femoral canal is enlarged, and the femoral stem is inserted with or without the use of synthetic cement. A trial reduction of the hip follows, along with the assessment of its length and stability. Finally, the selected head is placed, and the hip is definitively reduced. The wound is sutured, and the patient is transferred to the recovery room. The duration of the surgery ranges between 45 and 60 minutes.
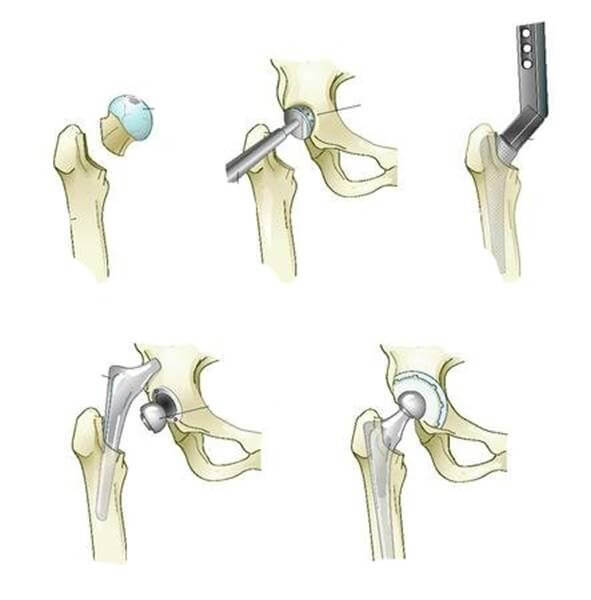
The steps of total hip arthroplasty.
What happens after the surgery?
The patient stays in the recovery room for about one hour. Bed mobilization begins on the afternoon of the surgery day, while walking with the supervision of physiotherapists is required the next day. Antibiotics are administered for a duration of 48 hours, during which the presence of a urinary catheter is also necessary. The hospital stay lasts 3 to 4 days. The use of crutches is necessary for 4 to 6 weeks after the surgery.
Is the surgery painful?
With the use of epidural analgesia, the surgery is almost painless.
After discharge from the hospital, anticoagulants are necessary, administered either by injections or preferably tablets, for a period of 3 weeks.
When is driving allowed?
It is recommended to avoid driving for 4 to 6 weeks, or until control of lower limb movements is fully restored. The exact timing is determined by the surgeon.
What are the risks and complications of hip arthroplasty?
As with any surgery, the following complications can occur after hip arthroplasty: venous thrombosis, infection, dislocation, and loosening.